Communication Connections: Enhancing Social Interactions for Autistic Children

A clinician I know, who runs an early-intervention practice, told me about an intake meeting she had not long ago. The parents had just been handed a four-year-old's diagnosis and were already asking which social skills training autism program to enrol him in. She told them, kindly, that the honest answer was: it depends, the evidence is real but smaller than the marketing implies, and the next conversation should probably not be about a curriculum at all.
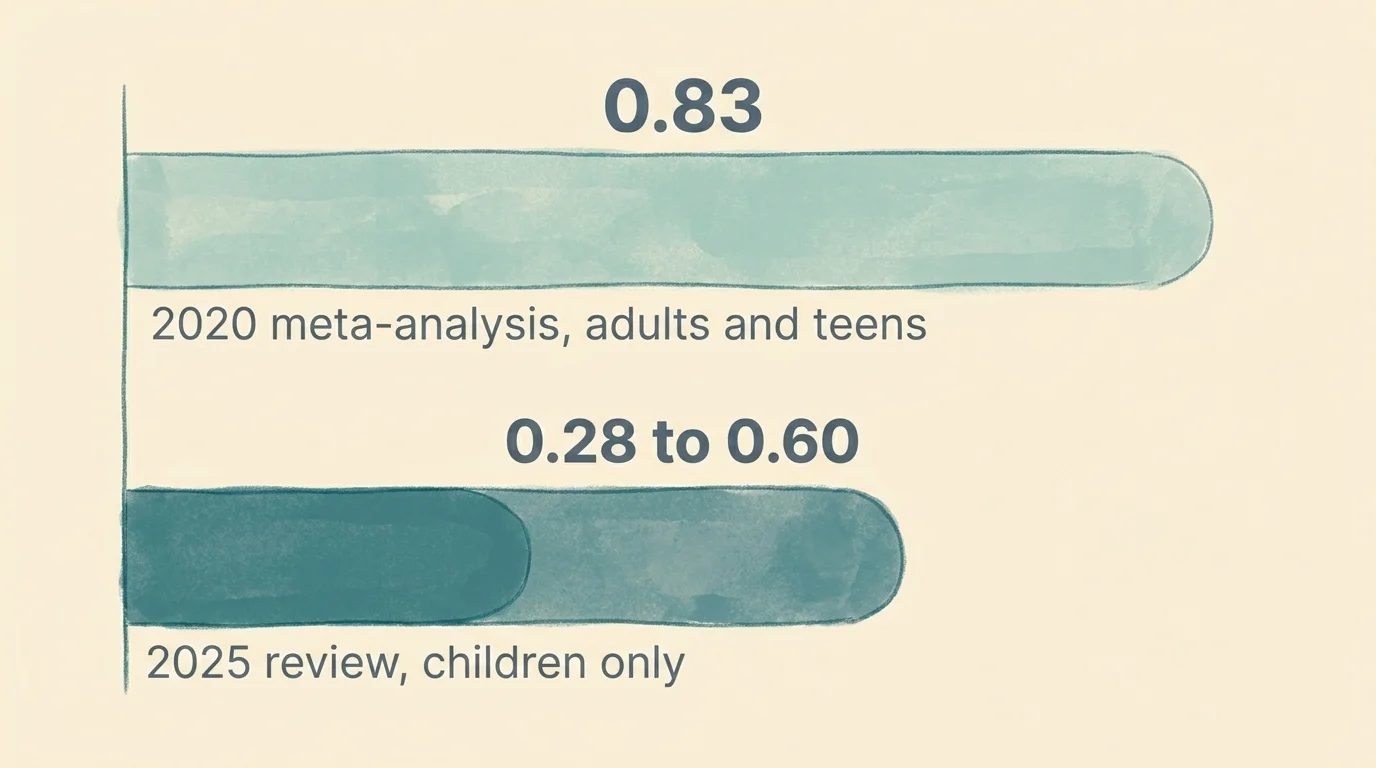
Here is a number that should be more famous than it is. A 2020 meta-analysis of 18 randomised controlled trials, with 1,266 autistic participants, found that social skills training for autistic learners produced an overall effect size of g = 0.83 — what statisticians call medium-to-large. That is a real result. It is also the high end of the range. A 2025 children-specific meta-analysis of 17 RCTs in the Saudi Medical Journal put the effect somewhere between 0.28 and 0.60, with the strongest gains in social communication, reciprocity, and joint attention. Both are correct. Both are talking about real children. The fact that the two numbers are so different is most of what you need to know before you choose what to do next.
Most articles about social skills training for autistic children are written as if the question is which five-step plan to follow. This one is not. The boring version of this piece, which I will repeat at the end, is roughly: the evidence supports specific named programs, in specific age ranges, for specific goals, as one part of a wider plan — and almost everything else is marketing.
The double empathy problem, before anything else
Before you spend any money or time on a curriculum, it helps to know that the framing of the whole field has shifted under it. For roughly thirty years, social skills training was built on the assumption that an autistic child was the party who needed to learn the rules. The clinical term was "social skills deficit." Most of the older literature still reads that way.
That assumption has been quietly demolished by a line of research starting with Damian Milton in 2012 and Sasson and Morrison's 2019 work, which found something inconvenient. When autistic adults talk to other autistic adults, they share information about as fluently as non-autistic adults talk to other non-autistic adults. The breakdown is between groups, not inside one of them. This is the double empathy problem: the misunderstanding is bidirectional, not a unilateral autistic deficit. Researchers call it a problem; in practice it is a correction.
This matters for two reasons. First, it changes which goals are reasonable. "Help my child read autism social cues from non-autistic peers" is a defensible goal. "Train my child to mask until they look non-autistic" is not, and a growing share of clinicians will say so to your face. Second, it changes who the work is for. If the misunderstanding is mutual, then teachers, classmates, and adults need some of the same scaffolding the child does. Almost no commercial program prices this in.
The programs you'll hear about
Most of the noise in this niche is generated by maybe a dozen named approaches. The 2025 narrative review in Translational Pediatrics categorised 21 distinct interventions into four evidence tiers and concluded that only two categories — CBT-based programs and naturalistic interventions — had substantial supporting evidence. The list below is the practical subset, in the order you are most likely to encounter them.
- PEERS (Program for the Education and Enrichment of Relational Skills). UCLA's 16-week structured social skills curriculum autism clinicians most often name first. Originally designed for autistic teens and young adults, with adapted versions for school-age children and a separate dating module for older participants. Highest-evidence CBT-based program in the 2025 review.
- Pivotal Response Treatment (PRT). A naturalistic, child-led approach that builds social motivation rather than drilling discrete skills. Strong evidence base; usually delivered by a trained therapist alongside parent coaching.
- LEGO® Therapy. Children build sets in assigned roles (engineer, supplier, builder), which forces collaboration. Moved from anecdotal to research-backed in the 2025 review.
- Social Stories™. Carol Gray's structured short narratives that describe a social situation and the expected sequence of actions. Useful as a scaffolding tool, especially for school-age children; not a standalone program.
- Video modeling. The child watches a short video of a peer or self performing a target social behaviour, then practises it. Cheap, well-studied, and underused.
- AAC and PECS. Augmentative and alternative communication systems — picture exchange, speech-generating devices, communication apps — that give non-speaking and minimally speaking children a way to participate in interactions while the rest of the work happens. Not a "social skills program" by name, but the foundation that makes everything else possible.
- ABA (Applied Behavior Analysis). A broader behaviour-change framework that may include social skills work but is not the same thing. Some ABA-derived social skills programs are well-evidenced; others are exactly the compliance-focused training that the neurodiversity-affirming critique is pointing at. Worth distinguishing program from framework.
Where do I actually start? A stage-by-stage outside view
No major competitor in this niche segments by developmental stage cleanly, which is strange because the answer to "where do I start?" is almost entirely a function of age. Treat what follows as the outside view: not a personalised plan, but the base rate of where the literature points first at each stage.
Toddler (roughly 18 months to 4 years)
Joint attention, gestures, and AAC supports if speech is delayed. The work at this age is rarely a curriculum and almost always a daily-life practice — pointing, sharing eye gaze with an object of interest, building a vocabulary of gestures and pictures the child can use to participate in the room. PRT and parent-mediated naturalistic interventions are the literature's strongest cards here. If your child is non-speaking or minimally speaking, AAC is not "what you do if speech doesn't come" — it is what you do alongside speech work, often from the start.
School-age (roughly 5 to 11)
Structured peer-play work, Social Stories™ for specific recurring situations (cafeteria, group projects, recess), and LEGO Therapy if a clinician offers it. Video modeling fits well at this age and costs almost nothing. School-age is also when most parents first hit the question of whether to use the school's social skills curriculum or pay for a private one. The 2024 Scientific Reports review on transferability of social skills training is the relevant data point: skills transfer better in mild autism than moderate autism, and duration, intensity, and context all matter — meaning a once-a-week pull-out group is doing less than a parent might assume.
Teen (roughly 12 to 18)
PEERS is the obvious recommendation here. It was designed for this stage, the evidence base is the strongest in the field for any single program, and it covers the social geography teenagers actually live in — friendships, group entry, electronic communication, conflict, and (for older teens) dating. If a clinician in your area runs PEERS, that is the conversation to have first.
Young adult
PEERS again, in its young-adult version, plus workplace-facing scripts and conversation rehearsal. The literature here is thinner than at any other stage, which is a polite way of saying it is mostly absent. Most young autistic adults are paying out of pocket for ad-hoc work, often in coaching rather than clinical settings.
The honest version of this stage map: the evidence is best for teens, defensible for school-age children, foundational for toddlers, and mostly improvised for young adults. If anyone tells you otherwise, ask them to name the studies.
Nonverbal communication: more than picture cards
The original version of this article folded nonverbal communication into a single paragraph about picture cards and basic gestures. The current scope is wider. Searches for "nonverbal communication autism" have actually risen 23 per cent in the most recent month, against a longer downtrend, which suggests the topic is having a quiet revival driven by AAC adoption.
The practical version: nonverbal communication is a system, not a workaround. It includes a child's gestures, eye-gaze patterns, facial expressions, and body orientation, plus any AAC scaffolding — picture exchange systems, speech-generating tablets, communication apps. A speech-language pathologist can audit which of these your child is already using fluently and which are missing. Visual supports — schedules, social stories, choice boards — sit alongside the AAC work; they are not a substitute for it. None of this is in tension with verbal speech work; the older idea that AAC delays speech has not held up, and most current SLPs treat it as additive rather than competing.
Conversations through shared interests, with one honest caveat
Special interests are the most reliable conversation anchor most autistic children offer their families and teachers. The standard advice — follow the child's lead, ask genuine questions about their interest, use it as a structured prompt — is correct as far as it goes. Sasson and Morrison's bidirectional communication finding suggests one extension of it: when an autistic child has a chance to talk to other autistic children with overlapping interests, the conversational fluency that often looks "missing" in mixed-group settings reliably appears. If your child has a special interest, the cheapest social skills intervention available may be finding two or three other children who share it.
Technology: the part the marketing is right about
Behavioural intervention technologies — avatars (FaceSay), emotion-recognition software (Mind Reader), therapeutic robots like iRobiQ and CARO — were once treated as second-best to face-to-face training. The 2020 meta-analysis killed that assumption. Tech-based programs produced an effect size of g = 0.93, face-to-face training g = 0.81; the difference was not statistically significant. Whatever else this means, it means tech-delivered SST is not a downgrade.
Social skills apps autism-focused families actually use are usually a mix of two categories: structured practice apps (FaceSay, Conversation Builder, Social Express) and communication tools that double as social practice environments (Proloquo2Go, AAC apps that scaffold turn-taking). VR practice environments and AI-driven progress tracking are entering clinical use as of 2025 and are worth watching, though they are not yet standard.

Does any of this actually work? The numbers.
Two effect sizes worth knowing. The 2020 Lim et al. meta-analysis reported an overall g = 0.83 across 18 RCTs and 1,266 participants — medium-to-large. The 2025 children-specific review in the Saudi Medical Journal, looking at 17 RCTs of children aged 3 to 18, found a smaller range of 0.28 to 0.60. Both are real. The most likely explanation for the gap is the population: the 2020 analysis included older adolescents and young adults, where the evidence is strongest; the 2025 analysis is children-only, where transfer to real-world settings is harder.
The takeaway is not that one number is right and one is wrong. It is that the honest expected effect, for a school-age autistic child enrolled in a well-delivered program, sits somewhere in the middle — small to moderate, not transformative. That is still worth doing. It is not a cure, and any program describing itself as one is selling something else.
What the research says NOT to do
The 2025 narrative review's caveat is worth reading carefully: social skills training, the authors write, should be "one component of a broader, individualized treatment plan" rather than a standalone intervention. The neurodiversity-affirming critique, summarised most clearly by the Therapist Neurodiversity Collective, goes further: programs whose goal is compliance, masking, or making the child appear non-autistic are now openly criticised by clinicians inside the field, not only by autistic self-advocates outside it. You do not have to take a side in that debate to take its main practical point: when you evaluate a program, ask whose comfort it is optimising for.
A note on cost
Most American families pay for at least part of social skills training out of pocket. The first peer-reviewed cost analysis of SST, published in Sage's Autism journal in 2026, found that families bear the largest share of the cost burden, though per-child implementation costs are lower than many other autism interventions. School-based programs are the obvious cheaper alternative; their fidelity to the named curricula varies a great deal.
The boring version of this advice
For toddlers and school-age children, naturalistic and parent-mediated approaches plus AAC where speech is delayed; for teens, PEERS if you can access it; for everyone, treat the curriculum as one component of a broader plan and ask what comfort the program is optimising for.
This advice will not help if the goal is a cure, if the program is delivered by someone who has not read the post-2019 literature, or if the family does not have the bandwidth to do the at-home work the evidence assumes. In those cases the conversation that matters is not which program to choose; it is which support the family needs first.
Frequently Asked Questions
A speech-language pathologist can audit the gestures, eye-gaze patterns, facial expressions, and AAC scaffolding (picture exchange systems, speech-generating tablets, communication apps) a child is already using and identify what is missing. Visual supports — schedules, social stories, choice boards — sit alongside the AAC work, not as a substitute for it. The older idea that AAC delays speech has not held up, and most current SLPs treat it as additive.
Use the child's special interest as the conversation anchor — follow their lead, ask genuine questions, and offer structured prompts on familiar topics. Sasson and Morrison's 2019 finding suggests an extension: when an autistic child has the chance to talk to other autistic children with overlapping interests, conversational fluency that often looks 'missing' in mixed-group settings reliably appears.
A 2020 meta-analysis found that technology-based social skills programs produced an effect size of g = 0.93, statistically equivalent to face-to-face training (g = 0.81). Avatars (FaceSay), emotion-recognition software (Mind Reader), therapeutic robots, and AAC apps that scaffold turn-taking are all in active use; VR practice environments and AI-driven progress tracking are entering clinical use as of 2025.
A 2020 meta-analysis of 18 RCTs and 1,266 participants found a medium-to-large effect (g = 0.83). A 2025 children-specific review of 17 RCTs (ages 3–18) in the Saudi Medical Journal found a smaller range of 0.28 to 0.60, with the strongest gains in social communication, reciprocity, and joint attention. The honest expected effect for a school-age child in a well-delivered program is small to moderate — real, but not transformative.
PEERS (Program for the Education and Enrichment of Relational Skills) is UCLA's 16-week structured social skills curriculum, originally designed for autistic teens and young adults, with adapted versions for school-age children and a separate dating module for older participants. The 2025 narrative review in Translational Pediatrics rates it among the highest-evidence CBT-based programs in the field.
There is no single right age — the literature points to different work at each stage. Toddlers benefit from joint attention, gestures, and AAC if speech is delayed; school-age children from Social Stories, peer-play work, and LEGO Therapy; teens from PEERS; young adults from PEERS' young-adult version plus workplace scripts. The 2024 transferability research suggests skills transfer better in mild autism and that intensity, duration, and context all matter.
No. ABA (Applied Behavior Analysis) is a broader behaviour-change framework that may include social skills work. Social skills training is also delivered through CBT-based programs (PEERS, summerMAX), naturalistic methods (Pivotal Response Treatment, LEGO Therapy), and parent-mediated approaches. The 2025 narrative review in Translational Pediatrics identifies CBT and naturalistic interventions as having the strongest evidence.
A research-backed reframe (Milton 2012; Sasson and Morrison 2019) showing that social misunderstandings between autistic and non-autistic people are bidirectional, not a one-way autistic deficit. It is reshaping how clinicians design social skills programs to focus on mutual communication rather than asking autistic children to mask.