Understanding Autism Spectrum Disorder: An In-Depth Exploration

A parent I met at a conference once told me, with the slightly bewildered honesty of someone who has been reading the internet, that she had spent three months trying to work out whether her son was "high-functioning" or "low-functioning" before realising she had no idea what the question meant. The clinical reports she had read used different words again. The autistic adults whose blogs she had been reading had a third vocabulary, and they were the ones who told her, kindly, that the original question was the wrong one.
This essay is a current-research overview of autism spectrum disorder — what the term means, what the language conventions are, what the 2025 research has begun to show about the structure of autism itself, what the early signs look like across ages, when an adult might recognise themselves in the description, and where to go next. It is written for parents of newly-identified children, for adults who are recognising themselves in the literature, and for anyone trying to make sense of the vocabulary the field is currently in the middle of revising.
A note on what this is. I am a clinical psychologist; I am not your diagnosing clinician. A formal autism diagnosis comes from a psychologist, psychiatrist, paediatrician, or developmental specialist with autism-specific diagnostic experience. This piece is an explainer that respects the boundary between explanation and assessment. Where the research is well-evidenced I will say so; where it is contested or unfinished I will say that too.
A note on language: identity-first and person-first
Two conventions exist in the literature. Identity-first language — autistic person — is preferred by a substantial majority of autistic adults in survey research and is the convention I will use here. Person-first language — person with autism — was preferred in clinical training in the 1990s and 2000s and is still the convention in some medical journals. Both are defensible; the difference matters because the convention you use signals which community you have been listening to.
A small caution from the consulting room: the families I see are sometimes told their language preference is wrong by people who have not asked which they would prefer. Both conventions exist for principled reasons. The work, in my experience, is to ask each autistic person you write or speak about which they prefer, and to default to identity-first when speaking generally.
The terminology: ASD, Asperger's, autism
A few short clarifications, because the search engine sees roughly 165,000 monthly queries for Asperger syndrome alone and many of those readers are working with a vocabulary the clinical literature has moved past.
- Autism spectrum disorder (ASD) is the current diagnostic category in the DSM-5 (the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, published in 2013). Most clinical writing now uses the term autism and autism spectrum disorder interchangeably.
- Asperger syndrome was a separate diagnosis in the DSM-IV (1994). When the DSM-5 was published in 2013, Asperger's, PDD-NOS, and several adjacent diagnoses were merged into the single ASD category. People diagnosed with Asperger's before 2013 still carry that diagnosis on their records; it is no longer issued as a new clinical diagnosis.
- PDD-NOS (Pervasive Developmental Disorder, Not Otherwise Specified) was likewise merged into ASD in 2013.
The reason for the merge was that the diagnostic boundaries between these conditions were not stable in research — different clinicians applied them differently, and the underlying biology and developmental trajectories did not cluster neatly along the old category lines. The DSM-5 collapsed them into a single category with severity-based modifiers, which has its own problems but at least removes the false precision of the older labels.
Levels of support, not functioning labels
The DSM-5 introduced three levels of required support for ASD (CHOP's Center for Autism Research summary is the cleanest reference):
- Level 1 — requiring support. Difficulties in social communication and inflexibility cause noticeable difficulty in everyday life without support, but the person is largely independent.
- Level 2 — requiring substantial support. Marked difficulties in social communication; inflexibility limits functioning across multiple contexts.
- Level 3 — requiring very substantial support. Severe difficulties in social communication and severely inflexible behaviour that markedly limit functioning.
I want to say something careful about the older language these levels are slowly replacing. The terms high-functioning autism and low-functioning autism (or severe autism) were never formal diagnoses. They were shorthand. They are also, in the experience of most autistic adults I have met or read, reductive in a particular way: they describe how a person looks to non-autistic observers more accurately than they describe what the person is doing internally or how much support they need across different domains.
A widely-cited example: an autistic person fluent in conversation may be exhausted by the masking that produces the fluency, may struggle with executive function in ways that fluency hides, and may need substantial sensory accommodation that no observer would predict from the conversation. High-functioning misses all of this. The DSM-5's requiring substantial support misses less of it because it asks about support needs across several domains, but even the levels framework has been criticised in the academic literature for forcing a qualitative reality into a quantitative scale.
The honest version, I think, is this: any single label about an autistic person's "level" is doing summary work that a multi-axis description (social, communication, sensory, executive, motor, restricted interests) does much better. The DSM-5 levels are an improvement on functioning labels and not a substitute for the longer description.
Cleveland Clinic's current autism page avoids functioning labels entirely. It is worth noting that the major medical centre's editorial choice and the autistic community's preference are now in the same place; the slower-moving parts of the field will catch up.
The 2025 subtypes finding
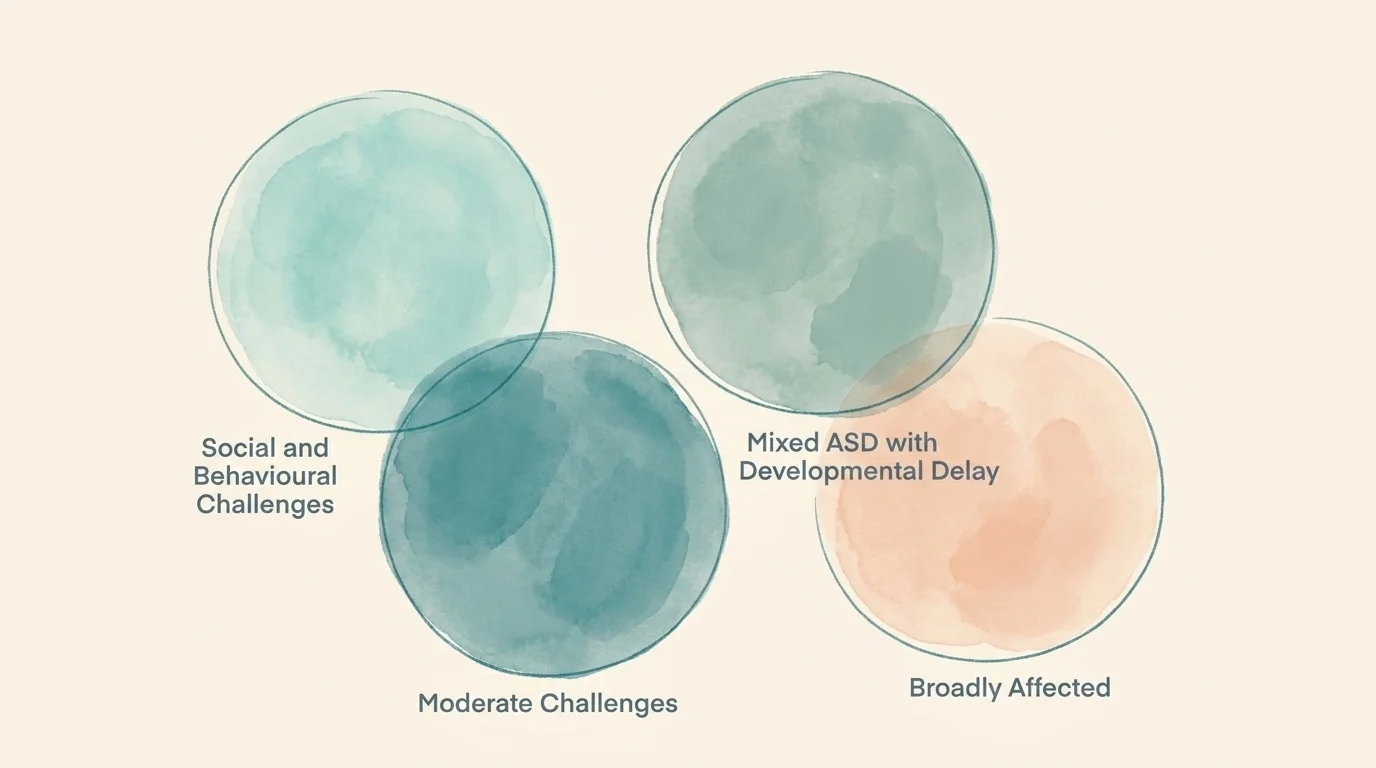
In July 2025, a Princeton-led team led by Olga Troyanskaya, working with the Flatiron Institute, published a paper in Nature Genetics (Princeton's news summary is more accessible) that has begun to change how thoughtful clinicians describe the structure of autism. They analysed data from 5,392 children in the SPARK cohort and identified four biologically distinct autism subtypes:
- Social and Behavioural Challenges
- Mixed ASD with Developmental Delay
- Moderate Challenges
- Broadly Affected
Each maps to distinct genetic profiles and developmental trajectories. The implication, restated carefully: the linear-spectrum metaphor that has organised most popular writing on autism for two decades is, in genetic terms, an oversimplification. There is more than one autism, and the subtypes have different biological substrates.
This is one paper, on one cohort, in one journal. A small caution from the consulting room: large studies with this kind of headline finding tend to look smaller in the second and third replication studies than they did in the first publication. The subtypes are not yet a clinical instrument and should not be treated as one. But the direction of the finding — that "the spectrum" is closer to several overlapping spectra than to a single linear one — is consistent with what most experienced clinicians have informally observed for years, and it is the strongest 2025 challenge to the older language.
How common is autism in 2026
The most recent CDC figures, from the April 2025 ADDM Network release (surveillance year 2022), put US autism prevalence at 1 in 31 children identified by age 8 — about 3.2 per cent. This is up from 1 in 36 in the prior cycle and from 1 in 150 in the year 2000. Boys are diagnosed at roughly 49.2 per 1,000 versus girls at 14.3 per 1,000, a ratio of about 3.4 to 1. Median age of diagnosis is 47 months.
The natural question this raises — is autism becoming more common? — has a more interesting answer than the headline implies. The current scholarly consensus, summarised carefully by Johns Hopkins Bloomberg School of Public Health, is that most of the prevalence increase reflects screening reach catching up to existing autistic people. Asian, Black, Hispanic, and multiracial children are now diagnosed at rates that match or exceed white children in some areas — a reversal of historical disparities. The finding is consistent with autistic people having always existed in the population at roughly the current rate; what has changed is the clinical infrastructure for identifying them. The "epidemic" framing common in older media coverage is, on the available evidence, the wrong frame.
For adults the picture is fuzzier but moving fast. The CDC estimates roughly 1 in 45 US adults is autistic, with substantial undercount expected. JAMA Network Open in 2024 documented a 450 per cent increase in autism diagnoses among adults aged 26 to 34 between 2011 and 2022. The most likely explanation, again, is recognition rather than incidence — the diagnostic criteria broadened in 2013, public awareness of how autism presents in adults (especially in girls, women, and people who have learned to mask) caught up over the next decade, and many adults who would have been missed in childhood are now arriving at clinics.
Recognising autism in adulthood
The fastest-growing segment of autism diagnosis in 2025 and 2026 is adults. The clinical pattern that brings adults to assessment is, in my experience, fairly consistent across the people I have seen. A recurring theme of social effort that has felt different from peers' for a long time. Sensory experience that has always been more intense, more dampened, or more inconsistent than friends and family seem to manage. Patterns of focused interest that have been productive in some seasons of life and exhausting in others. A history of burnout that does not quite match what generic burnout literature describes.
Several signposts that consistently show up in the adult-diagnostic literature (Yale Medicine has a good overview):
- Long-standing social-communication differences. Often described in retrospect as always feeling like I was performing in social situations.
- Sensory differences. Hypersensitivity, hyposensitivity, or both — to sound, light, texture, smell, temperature.
- Intense focused interests. Often productive; sometimes the source of professional accomplishment; sometimes a source of conflict with employers or partners who interpret them as obsession.
- Masking burnout. A particular kind of exhaustion that comes from sustained social performance over a working day or week.
- A history of being told you are too sensitive, too rigid, too intense, or too much.
Adult diagnosis runs through a clinical psychologist or psychiatrist with autism-specific experience, often involving structured interviews (the ADOS-2, the ADI-R, or adult-adapted variants), self-report measures (the AQ, the RAADS-R), and a developmental history. Many adults find the assessment itself useful even when the clinical conclusion is uncertain; the conversation forces a structured retrospective look at one's own life that is rare to come by otherwise.
A small note on co-occurring concerns. Adult autism diagnosis often coincides with anxiety, depression, or burnout that has been present for years. If you are in crisis or experiencing thoughts of self-harm, contact a national crisis line first; the diagnostic conversation can wait, the safety conversation cannot.
Signs across ages: a quick reference
The CDC's Learn the Signs. Act Early milestones are the standard reference for early detection; what follows is a working summary by developmental stage rather than a substitute for those milestones. The CDC notes that ASD can be detected at 18 months or younger, and that a diagnosis by an experienced professional is considered reliable from around age 2.
By 18 months. Limited or absent pointing to share interest; limited eye contact; few or no words; limited response to name. Strong reactions to certain sounds, textures, or routines.
By 2 to 3 years. Few words or unusual word use (echolalia, scripting from media); limited pretend play; intense focused interests; lining up or sorting objects rather than playing functionally with them; significant distress at change in routine.
By school age. Difficulty with peer interaction in unstructured settings; literal interpretation of language; intense special interests; sensory accommodations needed for noise, light, or texture; difficulty recognising or naming emotions in self or others.
In adolescence and adulthood. See the prior section. The adult presentation often involves a long-standing experience of social effort, sensory difference, and masking burnout that may have been mislabelled (anxiety, depression, ADHD, "highly sensitive person," "introversion") for years.
If you recognise your child or yourself in any of these descriptions, the next step is not the internet. It is a conversation with your paediatrician or GP about a referral to a developmental specialist or autism-specific assessment service.
Sensory differences and stimming, briefly
Two features of autistic experience that are widely recognised in the community and in current research, but often described thinly in popular explainers:
Sensory differences — hypersensitivity, hyposensitivity, or both — affect a substantial majority of autistic people across hearing, vision, touch, taste, smell, balance, and proprioception. The 2025 systematic-review literature treats sensory integration occupational therapy as evidence-based for autistic children aged roughly 4 to 12, and the broader pattern of sensory accommodation (quiet spaces, predictable lighting, noise-reducing headphones, weighted blankets, fidget tools) is now standard in most well-designed autism-friendly environments.
Stimming — repetitive sensory or motor self-regulation behaviour — is now consistently described in the affirming literature as functional rather than pathological. It serves arousal regulation, emotional regulation, attention focus, and pleasure. The current consensus, summarised in the 2024–2025 neurodiversity-affirming literature, is that suppressing stimming through masking directly raises the risk of meltdown and shutdown by depleting the cognitive and emotional resources the person has available. Allow stimming unless a specific stim is dangerous; redirect only when it endangers the person.
Diagnosis and early intervention
Early intervention is, on the available evidence, one of the more consistently supported domains in autism research. The reasoning is straightforward — earlier engagement allows more developmental time for skill-building and accommodation — and the practical implication for parents is that a referral pathway initiated soon after concern is raised is worth more than a long wait for the perfect specialist.
In the United States, the relevant pathways are:
- Birth to 3 years. Early Intervention services under IDEA Part C — referral typically through your paediatrician or directly through your state's Early Intervention programme.
- 3 to 21 years. Special education services under IDEA Part B, accessed through your local school district. Parents can request an evaluation in writing.
- Outside the school system. A developmental paediatrician, a clinical psychologist, or a multidisciplinary autism diagnostic team (often based at a children's hospital). Wait times vary considerably by region; the Child Find provision of IDEA obligates the school district to identify and evaluate children with suspected disabilities at no cost to families.
The interventions with the most consistent evidence base in 2025 cover speech-language therapy, occupational therapy (including OT-led sensory integration), naturalistic developmental-behavioural interventions (including Pivotal Response Treatment and the Early Start Denver Model), and structured social skills programmes appropriate to the child's age. Applied Behaviour Analysis (ABA) remains the most widely-funded behavioural intervention but is also genuinely contested in the autistic community; if it is recommended for your child, the question worth asking is which of the several modern variants the practitioner uses and how compliance-focused the programme is.
When and where to seek a diagnosis
If you suspect autism in your child or yourself, the practical next steps are:
- For a child. Talk to your paediatrician or GP about a referral. In the US, request an evaluation in writing from your local school district under IDEA, in parallel with the medical referral. Both pathways move slowly; starting both at once is often the most efficient approach.
- For an adult. Seek a clinical psychologist or psychiatrist with adult-autism diagnostic experience. Some primary care physicians can refer; some adults self-refer to a specialty practice. Insurance coverage varies considerably; many adults pay out-of-pocket for the assessment.
- For both. Bring a developmental history. For children, school records and any prior evaluations. For adults, a written narrative of long-standing patterns is often more useful than the assessment instruments alone.
The diagnosis itself is one piece of a longer process. What it gives you, in my experience, is access — to services, to accommodations, and most usefully, to a community that has been thinking about how to live well with the same nervous system you have. The wait for the assessment is sometimes long. The framework for understanding what the assessment will say is, in 2026, more robust than it has ever been.
The honest version
Most of what is true about autism in 2026 was true twenty years ago and is only now being measured carefully. The terminology is in revision. The functioning labels are quietly being retired. The research has begun to describe several biological patterns rather than one. Adult diagnosis is the fastest-growing part of the picture and the part most poorly served by older popular writing.
The work, for parents and for newly-identified adults alike, is not to find the right label. It is to find a description rich enough to live inside, a clinician careful enough to notice what the description leaves out, and a community whose vocabulary leaves room for what the description is still in the middle of becoming.
Frequently Asked Questions
Autism spectrum disorder is the current diagnostic category in the DSM-5 (2013) describing a developmental difference in social communication, sensory experience, and patterns of interest and behaviour. The terms 'autism' and 'autism spectrum disorder' refer to the same diagnosis. Most clinical writing now uses them interchangeably. The CDC's most recent surveillance data (2022, published April 2025) identifies autism in 1 in 31 US children at age 8.
Since the DSM-5 was published in 2013, the two terms refer to the same diagnosis. The DSM-5 merged previously separate diagnoses — including Asperger syndrome and PDD-NOS — into a single ASD diagnosis with three severity levels. The reason for the merge was that the diagnostic boundaries between the older categories were not stable in research.
The DSM-5 defines three levels of required support. Level 1 — requiring support: difficulties cause noticeable difficulty in everyday life without support, but the person is largely independent. Level 2 — requiring substantial support: marked difficulties in social communication, inflexibility limits functioning across contexts. Level 3 — requiring very substantial support: severe difficulties in social communication and severely inflexible behaviour. The levels describe support needs, not personal 'functioning.'
Clinical guidelines have largely moved to DSM-5 support levels, and many autistic adults reject functioning labels as reductive. They describe how a person looks to non-autistic observers more accurately than they describe what the person is doing internally or how much support they need across different domains. Major medical centres (including Cleveland Clinic) now avoid the terminology.
Neurodivergent describes a person whose cognition differs from what a society treats as standard, including autism, ADHD, dyslexia, dyscalculia, dyspraxia, and Tourette syndrome among others. Neurodiversity is the broader concept that this variation in human cognition is a property of populations, not a deficit in individuals. The term was coined by Australian sociologist Judy Singer in 1998.
Adult autism diagnosis has risen sharply — JAMA Network Open reported a 450% increase among adults aged 26–34 between 2011 and 2022. Common signs include long-standing social-communication differences, sensory hypersensitivity or hyposensitivity, intense focused interests, masking burnout, and a history of being told you are too sensitive, too rigid, or too intense. Formal diagnosis comes from a clinical psychologist or psychiatrist with autism-specific experience.
The CDC notes that autism spectrum disorder can be detected at 18 months or younger, and that a diagnosis by an experienced professional is considered reliable from age 2. Earlier referral and engagement allows more developmental time for skill-building and accommodation; the practical implication for parents is that initiating a referral pathway when concern is raised is more useful than waiting for the perfect specialist.
The CDC's most recent surveillance data (April 2025 ADDM release, surveillance year 2022) identifies autism in 1 in 31 US children at age 8 — about 3.2 per cent. This is up from 1 in 36 in the prior cycle and from 1 in 150 in the year 2000. The current scholarly consensus, summarised by Johns Hopkins, is that most of the increase reflects improved screening reaching previously underserved groups, not a 'true' increase in incidence.
A Princeton-led team led by Olga Troyanskaya, working with the Flatiron Institute, published a paper in Nature Genetics in July 2025 identifying four biologically distinct autism subtypes — Social and Behavioural Challenges, Mixed ASD with Developmental Delay, Moderate Challenges, and Broadly Affected — each linked to different genetic profiles. The finding reinforces that autism is multi-axis, not a single linear spectrum. It is one cohort study and not yet a clinical instrument.